
Ivermectin is a well-known antiparasitic medicine used in human and veterinary medicine. In human care, its strongest established use is for selected parasitic infections, especially strongyloidiasis, onchocerciasis, and certain external parasite conditions such as scabies and lice. It is valued because it can work at very small weight-based doses, is usually simple to administer, and has a long record of use in parasite-control programs.
Ivermectin acts mainly on parasite nerve and muscle function. It binds to glutamate-gated chloride channels found in many parasites, increasing chloride flow into cells. This can paralyze or kill susceptible parasites. Humans do not have the same target channels in the same way, which is one reason ivermectin can be used safely at approved human doses when properly prescribed.
For strongyloidiasis, the DailyMed label for Stromectol lists a single oral dose designed to provide about 200 mcg/kg of body weight. For onchocerciasis, the listed dose is about 150 mcg/kg of body weight as a single oral dose. The same label notes that ivermectin tablets are taken with water on an empty stomach for those labeled uses.
A practical example:
At 200 mcg/kg, a 70 kg adult receives about 14 mg total. At 150 mcg/kg, a 70 kg adult receives about 10.5 mg total. Final tablet rounding depends on tablet strength and clinician judgment.
For classic scabies, oral ivermectin is used in some clinical settings even though U.S. labeling differs by indication. CDC clinical care guidance lists 200 mcg/kg per dose, usually as two doses taken 7–14 days apart, with food.
The strongest positive profile for ivermectin remains its parasite-related activity. For the right parasite, it can be highly useful, low-volume, and easy to administer compared with longer treatment schedules. It has been widely used in mass parasite-control programs, especially for onchocerciasis, where repeat community dosing reduces microfilarial burden and disease transmission.
In relation to cancer, ivermectin displays positive effects on cancer-cell behavior. Published reviews describe activity involving cancer-cell death pathways such as apoptosis, autophagy, and pyroptosis, along with effects on signaling pathways involved in growth, survival, migration, and resistance.
Recent studies have provided compelling evidence regarding Ivermectin’s mechanisms of action in cancer cells, demonstrating its capacity to modulate multiple oncogenic signaling pathways, including Wnt/β-catenin, PI3K/Akt/mTOR, and STAT3. These interactions contribute to apoptosis induction, inhibition of tumor cell proliferation, and modulation of the tumor micro environment across a range of malignancies.
Preclinical studies provide encouraging evidence of anticancer potential, showing that Ivermectin can reduce tumor volume by more than 50% in murine models, even at doses lower than the maximum safe limits defined for humans.
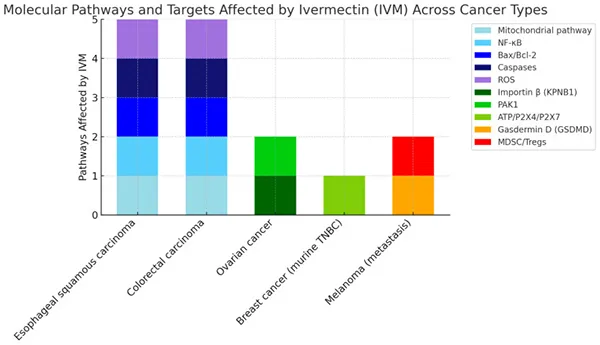
This shows the percentage of inhibition of specific molecular pathways in different types of cancer after treatment with Ivermectin. It summarizes the molecular mechanisms influenced by Ivermectin across several cancer models. Each stacked bar represents the number and type of pathways affected in a given cancer type, with colors corresponding to specific molecular targets: mitochondrial pathway (light blue), NF-κB (cyan), Bax/Bcl-2 (blue), caspases (dark blue), ROS (purple), importin β (KPNB1, light green), PAK1 (green), ATP/P2X4/P2X7 (yellow-green), gasdermin D (GSDMD, orange), and MDSC/Tregs (red).
Esophageal squamous carcinoma and colorectal carcinoma show modulation of five distinct pathways, suggesting a broad mechanism of action. In contrast, ovarian cancer, murine triple-negative breast cancer (TNBC), and metastatic melanoma involve fewer pathways, but still reflect targeted effects relevant to apoptosis, immune regulation, and tumor progression. This visualization highlights the pleiotropic and context-dependent actions of Ivermectin, supporting its potential role as a multi-target anticancer agent.
Other reviews describe effects involving PAK1, WNT/β-catenin, mitochondrial stress, and immune-related tumor changes. There is also human clinical research combining ivermectin with immune-based cancer treatment.
For post-COVID symptoms or “COVID injuries,” BSI has standardized ivermectin dosing for prescribing to various patient needs.
The positive way to frame ivermectin is this: it is a high-value antiparasitic drug with a large global history, simple weight-based dosing for several parasite conditions, and ongoing scientific positive results in immune, inflammatory, cancer, and viral-related fields. The strongest dosing confidence is for parasites.
Standard dose references include 200 mcg/kg for strongyloidiasis, 150 mcg/kg for onchocerciasis, and 200 mcg/kg repeated after 7–14 days for classic scabies when oral therapy is selected. For cancer and COVID-related injury, dosing per BSI standard prescription, based on patient needs.
When researching Ivermectin for Covid injuries and cancers, negative bias is endemic by design. Suppressed testimony and scientific investigation is difficult to find, but is available with persistent investigation. In our experience, Ivermectin, when combined with other therapies such as Mebendazole and a huge host of therapies available at BSI, positive healing results are possible.